|
Get AfricaFocus Bulletin by e-mail!
Format for print or mobile
USA/Africa: "Pro-Death" Health Agendas Advance
AfricaFocus Bulletin
May 30, 2017 (170530)
(Reposted from sources cited below)
Editor's Note
"3.3 million more abortions. 15,000 more mothers dying. 8 million more unplanned
pregnancies. ... Those grim numbers from the Guttmacher Institute show the potential
real-world impact of the Trump administration's unprecedented proposed cuts to global
family planning efforts; the budget the White House released Tuesday would basically
eliminate those programs." - Sarah Wildman, Vox, May 24, 2017
The headline (my wording) may seem alarmist, but detailed examination of the health
agendas being advanced by the Trump administration and right-wing Republicans leaves
little doubt of the consequences should they be fully implemented. There will indeed
likely be millions of deaths resulting both from the House domestic healthcare plan,
which would remove 23 million from health insurance, according to the Congressional
Budget Office, and from the provisions for global health in administration's new
budget. That would�eliminate funding for family planning, threaten funding for
HIV/AIDS and famine relief, and impose massive cuts on institutions such as the
Center for Disease Control which are vital to protection against epidemics.
One may withhold judgment on the motivations of the policymakers, including the
relative weight of ideology, indifference, lack of human empathy, and greed. And most
observers say the full package is unlikely to survive Congressional scrutiny, even
among many Republicans. But much of the damage, such as the Global Gag Rule cited
above, comes from executive decisions already being implemented, such as the new
version of the Global Gag Rule. The proponents of this agenda, it is clear by their
explicit statements, reject the universal right to health, and give little or no
value to the lives of those who are not wealthy and white.
This AfricaFocus Bulletin continues two summary articles on the Global Gag Rule and
the Trump budget, as well as a reflection on the pressures facing progressive health
advocates stretched by the attacks on both domestic and global health.
A few additional short articles highlight the threat:
Siobhán O'Grady, "How teen moms in Nigeria could wind up hurt by Trump's U.N. Cuts,"
Washington Post, May 5, 2017
http://tinyurl.com/y9dn2odb
Documents effects of cutting support for the U.N. Population Fund.
Los Angeles Times, "Editorial: Trump's new global gag rule will devastate healthcare
in poor countries," Los Angeles Times, May 22, 2017
http://tinyurl.com/n6kprqw
"The rule was bad enough in its earlier form [under previous Republican
administrations], when it barred aid to family planning organizations that offered
abortion or abortion counseling. ... But the new Trump administration incarnation of
the rule is far more expansive. ... it will now cover approximately $8.8 billion in
funds given out to healthcare providers of all sorts."
Nurith Aizenman, "Trump's Proposed Budget Would Cut $2.2 billion from Global Health
Spending," National Public Radio, May 25, 2017
http://tinyurl.com/y9xgbc87
"Overall, Trump would cut the annual global health budget by about 26 percent, or
around $2.2 billion in the 2018 fiscal year that begins October 1, decreasing it from
about $8.7 billion in the current fiscal year budget to less than $6.5 billion."
Emily Baumgaertner, "Proposed Cuts Alarm Bioterrorism Experts," New York Times, May
29, 2017
http://tinyurl.com/yavxmskg
The CDC's budget would be cut by 17%. At the NIH, a program training foreign medical
professionals in pandemic response would be eliminated.
For previous AfricaFocus Bulletins on health, visit
http://www.africafocus.org/intro-health.php
++++++++++++++++++++++end editor's note+++++++++++++++++
The Trump global gag rule: an attack on US family planning and global health aid
By Ann M. Starrs, Guttmacher Institute
The Lancet, February 4, 2017
http://www.thelancet.com � Direct URL: http://tinyurl.com/ya8ngh4h
On Jan 23, 2017, on his fourth day in office, President Donald Trump signed an
executive order imposing the global gag rule, an anti-abortion policy that under
other conservative presidential administrations has caused serious disruptions to US
overseas family planning efforts. Alarmingly, Trump's order goes even further than in
the past, with potentially devastating effect.
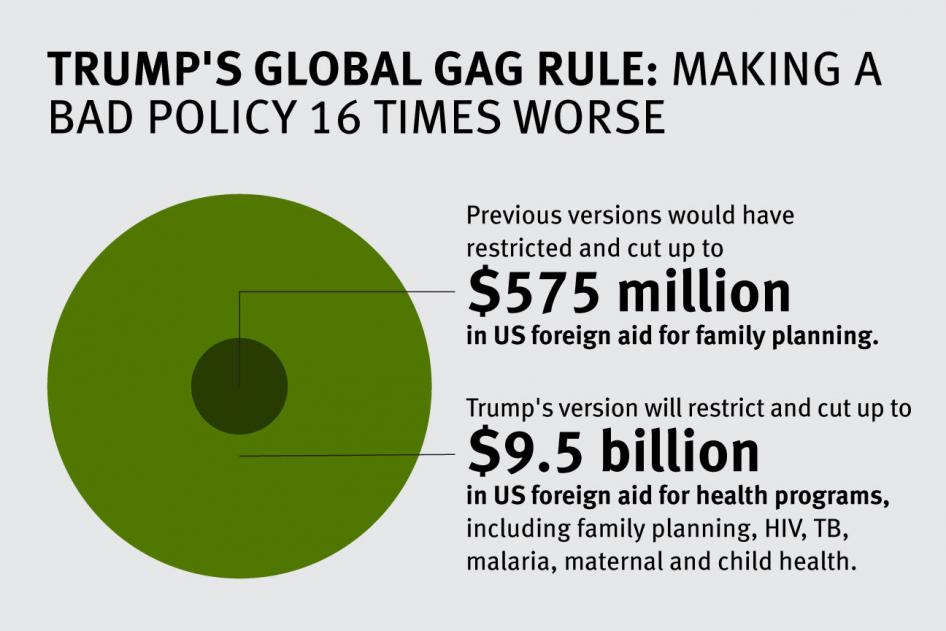
Credit for graphic: Human Rights Watch
The global gag rule, also known as the Mexico City policy, was devised in 1984 by the
administration of Ronald Reagan to impose a draconian set of anti-abortion rules on
US overseas family planning programmes. This policy banned US family planning funds
from going to foreign non-governmental organisations (NGOs) that provide abortion
services, counselling, or referrals, or advocate for liberalisation of their
country's abortion laws--even if they use non-US government funds for these
activities. In 1984, and every time the global gag rule has been imposed since then,
foreign governments were exempt for diplomatic reasons, as were US-based NGOs on
constitutional grounds.
To be clear, legislation was already in place in 1984, and is still in place now,
that bans the use of US funds under the Foreign Assistance Act from paying "for the
performance of abortion as a method of family planning". But for anti-abortion
activists this Helms Amendment, passed in 1973, did not go far enough; they wanted to
limit any activity that could possibly enable or promote abortion. Hence, the global
gag rule.
Under Trump's order, the gag rule now applies not only to US bilateral family
planning assistance (US$575 million for fiscal year 2016), but also to all "global
health assistance furnished by all departments or agencies"--encompassing an
estimated $9.5 billion in foreign aid. Foreign NGOs that receive US funding to work
on a broad range of health programmes in about 60 low-income and middle-income
countries--including on HIV/AIDS, the Zika virus, malaria, tuberculosis, nutrition,
and maternal and child health, among others--will potentially be subject to the same
ideological restrictions that have hampered family planning aid at points in the
past. Thus, President Trump's version of the global gag rule represents a wider
attack on global health aid writ large.
Adding to the widespread concern among US government agencies, global health NGOs,
and advocates is the Trump administration's failure to provide any guidance on the
interpretation or application of the new policy.
Those details may emerge in the coming weeks and months. But we already know that,
when last in effect, the gag rule crippled family planning programmes. Many foreign
NGOs, as a matter of principle and out of dedication to the patients they serve,
refused to let the US Government muzzle their abortion advocacy efforts or dictate
what services or counselling they provided using their non-US funds. These health
providers were forced to reduce staff and services, or even shut clinics. As a
result, many thousands of women no longer had access to family planning and
reproductive health services from these clinics--sometimes the only provider of such
services in the local community. Various actors, including the governments of Canada
and the Netherlands, are mobilising to compensate for at least some of the damage
that will be done by the gag rule. But the US is the largest funder of global health
programmes worldwide, and the disruption this aid effort will suffer is massive.
Moreover, there is no evidence that the global gag rule has ever resulted in its
stated aim of reducing abortion. The first study to measure the effect of the gag
rule showed that this policy could actually have resulted in an increase in
abortions. Another study assessed the gag rule in Ghana and found that because of
declines in the availability of contraceptive services, both fertility and abortion
rates were higher during the gag rule years than during non-gag rule years in rural
and poor populations. This is consistent with anecdotal data that the gag rule's main
effect has been to reduce women's access to quality contraceptive services, thereby
increasing the probability of unintended pregnancy and making recourse to abortion
more likely.
But the harmful effects of Trump's order are likely be even greater. NGOs in lowincome
settings often provide integrated health services; for instance, they offer
patients contraceptive care, HIV prevention or treatment, maternal health screenings,
immunisations, and information on safe abortion care all under one roof. By expanding
the gag rule to the full scope of US global health aid, hundreds more national and
local NGOs will be forced to choose between drastic funding cuts (if they decline to
sign the gag rule) or denying their patients the information and services that are
their right (if they sign, and can no longer provide or discuss abortion). Millions
of women living in low-resource settings may now be unable to obtain the care they
need, when they need it.
The unprecedented scope of the Trump global gag rule validates the fears of many
observers: reproductive health and rights worldwide will face a sustained attack in
the next 4 years of the Trump Administration. This assault will almost certainly
include defunding the United Nations Population Fund (UNFPA), as well as potentially
drastic cuts to US overseas family planning aid. It will be mirrored domestically by
efforts to restrict abortion access--for instance, by banning all private and public
insurance coverage of abortion or prohibiting the most commonly used method for
second-trimester procedures--and to shred the nation's family planning safety net,
including by defunding Planned Parenthood.
It is becoming clearer with each Trump executive order that not only reproductive
health but also global health programmes and overall foreign assistance supported by
the US Government are in grave jeopardy, as indicated by President Trump's repeated
promises to "put America first". The social conservatives driving this agenda--who
now control the US Presidency and both Houses of Congress--are showing complete
disregard for the millions of women, men, and children who will suffer the
consequences, intended or not, of these regressive policies.
Trump's budget eliminates US funding for global family planning and famine relief
by Sarah Wildman
Vox, May 24, 2017
http://www.vox.com � Direct URL: http://tinyurl.com/lrtqf72
3.3 million more abortions. 15,000 more mothers dying. 8 million more unplanned
pregnancies. Up to 26 million fewer women and couples acquiring contraception and
family planning advice.
Those grim numbers from the Guttmacher Institute show the potential real-world impact
of the Trump administration's unprecedented proposed cuts to global family planning
efforts; the budget the White House released Tuesday would basically eliminate those
programs.
It also calls for gutting a key US famine relief program, slashing half the budget
for the USAID's internal disaster relief organization, and cutting $222 million from
funds allocated to fight HIV, AIDS, tuberculosis, and malaria. The justification
listed in the budget is a simple hope for others to fill the shortfall:
The United States has been the largest donor by far to global HIV/AIDS efforts,
providing over half of global donor funding in recent years to combat this epidemic.
The Budget reduces funding for several global health programs, including HIV/AIDS,
with the expectation that other donors can and should increase their commitments to
these causes.
If Congress were to agree to those cuts (and that's a big if), advocates say the
global impact of America's abrupt departure from world health and disaster relief
would be immediate -- and devastating.
"The family planning elimination is the headline here," said Rachel Silverman, a
senior policy analyst on global health at the Center for Global Development. "It will
have the most impact on people's lives."
But Trump's proposed cuts to food aid and disaster relief would also deal a major
blow to some of the world's neediest and most desperate. Marilyn Shapley, a top
official at the aid group Mercy Corps, said some 70 million people need emergency
food assistance, while 20 million more are in famine-like conditions.
"This is going to take away food assistance from 33 million people in a year when
famine risk is higher than in decades," she said in an interview. "Before today I
wouldn't have thought it possible."
Funding family planning actually makes economic, not just moral, sense
This isn't the first time the Trump administration has taken aim at global family
planning and women's health.
In January, Trump reinstated the "Mexico City Policy," also known as the global gag
rule, which literally bars family planning providers from mentioning abortion in
their work. (The United States has long banned funds for abortion services.)
The policy is one that changes depending on the party of the president in power.
Obama immediately rescinded the policy when he moved into the White House; Trump,
like other Republican presidents before him, immediately reinstated it when he came
into office. As I wrote in January, the policy has traditionally limited the ability
of global family planning providers to give women and families comprehensive care if
in any aspect of their work they recommend, discuss, or even mention abortions to
clients, let alone provide abortion services.
But Trump went further than his predecessors. Previous Republican administrations
limited the policy to family planning providers; the Trump administration extended
the gag rule to all global health providers. That meant health care providers working
on everything from maternal and child health to malaria, tuberculosis, HIV/AIDS, and
vaccinations were now at risk of losing all US funding if they discussed abortion in
their work.
The NGO PAI estimated that the extended gag rule would affect about 15 times more US
funding than the gag rule had in the past. In mid-May, when the new rule went into
effect, Suzanne Ehlers, president and CEO of PAI, said Trump's move would do
"unspeakable damage to integrated care efforts."
That's a problem. With integrated care, a woman can come to a single clinic for, say,
vaccines for her children, then see a physician about her own contraceptive needs,
and finally seek advice, or refill prescriptions. In other words, she can meet all
her family's health care needs in one spot. For families traveling long distances, an
all-in-one clinic makes far more sense than one clinic for maternal health and
another for child care and still another for other medical services.
The Trump administration spent the first quarter of 2017 signaling plans to undermine
that sort of integrated care by reinstating the gag rule and beginning to reduce US
funding for maternal and infant health around the world.
In April, the administration announced it would strip the United Nations Populations
Fund (UNFPA), which works on reproductive health, family planning, HIV/AIDS, and
infant and maternal mortality in more than 150 countries, of all US funding. The
putative reason was a specious one.
"This decision is based on the erroneous claim that UNFPA �supports, or participates
in the management of, a program of coercive abortion or involuntary sterilization' in
China," a statement on the UNFPA website read. "UNFPA refutes this claim, as all of
its work promotes the human rights of individuals and couples to make their own
decisions, free of coercion or discrimination."
A State Department memo obtained by the Associated Press found no evidence that US
money had supported forced abortion or sterilization in China.
The decision costs the UNFPA $32.5 million in funding from the 2017 budget; the
United States was the fourth-largest donor to the organization.
The new budget would hit global health even harder.
Silverman noted that there's a "dissonance" between White House messages on women and
families. Ivanka Trump, the president's daughter, has claimed to be championing the
idea of women'e economic empowerment. That sort of program, Silverman says, would be
completely undermined by stripping global family planning from the budget.
"There is a lot of evidence that family planning contributes to women's empowerment,"
says Silverman, ticking off a list of things that planning, delaying, and spacing
pregnancies allow women to do -- like receiving an education, or even simply
advancing at work. "When women have control over fertility, they have control over
their lives."
Silverman points out that USAID directly funds 28 percent of contraceptives and
distribution in the developing world.
"If you cross-reference that with the number of women using contraceptives in those
countries -- a back-of-envelope calculation -- that suggests that 10 million women
are directly relying on USAID for contraceptives," she said, adding that enormous
numbers of women will "see a major disruption in their lives if this goes through and
other donors don't step up in a major way."
But there aren't other donors looking to step in. Jonathan Rucks, who runs PAI's
advocacy efforts, says there is no other donor government that can make up the
shortfall, and even major private family foundations, like the Bill and Melinda Gates
Foundation, simply cannot replace the US on family planning. In February, Bill Gates
told the Guardian that Trump's proposed reinstatement of the global gag rule could
"create a void that even a foundation like ours can't fill."
"If you are cutting maternal health funding, then you don't care about survival of
women," Rucks says bluntly. "We are also going to be really frank and say this is not
pro-life. This is undermining all your pro-life credentials."
Global Health in the Trump Era: Reflections on the Backlash
by Michelle Morse
Praxis, May 17, 2017
https://www.kzoo.edu/praxis/global-health-backlash/
Over the past thirty years, American medicine has witnessed an unprecedented
expansion in global health engagement amongst its trainees and faculty, partially, if
not largely, fueled by the health care injustices lived so dramatically by patients
in resource-limited countries around the world during the HIV/AIDS epidemic.
Initially seen as disruptive, the interventions in the health sectors of Global South
countries by American health professionals were eventually accepted as essential acts
in the movement towards achieving global health equity. As America experiences the
Trump era, endless questions have arisen amongst global health professionals about
the implications of Trump's "America first" platform on global health. Will Trump's
nationalist agenda eliminate funding for life-saving global health programs, cause
progressive health professionals engaged in global health to make a reactionary turn
towards the fire at home, and even force global health practitioners to more closely
examine their own prejudices?
It is no secret that American physicians leading the guard in global health tend to
be part of the political left. Global health tends to attract left leaning physicians
because of the global health movement's belief that every human being has a right to
receive high quality health care. Asserting that Global North countries have a
responsibility to contribute towards strengthening health care systems in the Global
South (a redistribution of resources, of sorts), global health offers the opportunity
to practically address urgent health care access inequities in the Global South.
Considering these principles, global health professionals like myself are deeply
frustrated by the Trump administration's efforts to repeal the Affordable Care Act
and cut global health spending at USAID and other similar programs. Though many of us
are rightfully drawn towards activism in the USA to resist these moves by the new
administration, I worry that the health and health systems of the Global South will
suffer if the majority of global health professionals shift to focus domestically
without continuing their engagement in global health.
While some would say that the current neoliberal structure of development aid is
already ineffective, especially since so many of the aid resources are actually
directed back to the country where the aid comes from, what would it mean if global
health funding was eliminated, and American global health professionals suddenly
focused exclusively on domestic health? Would it allow Global South countries to
assume stronger leadership, decision-making, and self-directed problem solving? Or
would it mean that Global South communities would be even more deprived of much
needed resources and health care access? Post-earthquake Haiti, where I have worked
for seven years and lived for two of those years, is one compelling example of both
the peril and the potential of aid. Of the $8 billion US funds provided in aid after
the earthquake, less than 1% went to the Haitian government who was ultimately
responsible for rebuilding the country. Yet, as appalling as this statistic is, it
does not adequately describe the individual impact of short- and long-term global
health engagement by American health professionals in response to the earthquake.
Take EqualHealth for example, the organization I co-founded. EqualHealth is a nongovernmental
organization focused on bringing light to the socially determined root
causes of illness and creating equity in opportunity for Haitian health professionals
whose talent and vision are often overshadowed by negative media narratives about
Haiti, weaknesses in the Haitian public health system, and limited opportunities for
professional development. All things considered, the reality is that countries like
Haiti rely on the shrinking aid from global health programs such as PEPFAR to keep
their health systems running despite fluctuations in attention from the donor world.
Where Global South countries would find themselves without USAID, or partnership with
Global North health professionals, or other mechanisms to ensure more adequate
resources for pressing health concerns is as predictable as where Americans, who rely
on the Affordable Care Act for health insurance, will find themselves when it is
repealed and replaced with a market-based solution.
What I have witnessed in my academic institution is an exciting and growing interest
amongst trainees in building infrastructure to resist the new administration's
domestic health care and civil rights policies. To mount a harmonized response, they
are looking into establishing indivisible chapters and partnerships with community
based organizations, learning and using direct action methods such as bird-dogging,
non-violent protest, and holding teach-ins on community organizing. These are often
the very same trainees that are also interested in global health. Though many of them
are considering careers in global health, opportunities for long-term global health
engagement with clear career paths and mentorship are often limited, and may now
become even more limited given the policies of the new American administration. On
the other hand, recent significant increases in donations to organizations like
Planned Parenthood could mean new opportunities for engagement for these trainees,
shaping careers focused on domestic health care. This is occurring at a time when
structural competency and social medicine are emerging as key areas of focus in
medical school and residency curricula, and trainees are being encouraged to engage
in activism as a professional obligation rather than aspiration. Health professionals
often hesitated to engage in activism as it was not an explicit part of their
training, and opportunities to act were difficult to identify, but these barriers
seem to be evaporating under the new administration.
In response to mounting evidence documenting how health care provider prejudice
impacts health, American medical schools are also developing competencies in which
trainees and faculty alike are encouraged to reflect on their personal biases. These
competencies are even more relevant now as the policies of this new administration
threaten the rights and livelihoods of people of color, women, Muslims, and
immigrants. Efforts to establish global health competencies, while laudable, have
often been silent on addressing the issues of racism, sexism, and other forms of
prejudice amongst global health professionals. The social and cultural power and
privilege clash that occurs when predominantly white global health professionals from
Global North countries descend on countries in the Global South to work hand in hand
with local health professionals who are predominantly people of color is a tinderbox
for racism and prejudice in all its forms. The global health movement can learn from
the new light being shed on the old problem of racism, as a result of the racist
policies and messages coming from the Trump administration in its first 100 days. The
global health movement needs to take the necessary steps to explicitly address racism
and other forms of prejudice amongst its members, and ask honest questions about why
more Americans of color are not currently a part of it. The far too common assumption
that being left leaning, progressive, or engaged in global health is incompatible
with being racist is simply incorrect.
As communities and countries in the Global South continue to suffer the consequences
of neoliberalism-induced fragile health systems, some global health professionals may
decide to deepen their engagement outside the USA, attempting to flee the
nationalist, racist, and sexist trends of the new administration by moving and
working abroad. Other global health professionals may decide to engage domestically
to resist the actions of the new administration, seeing the battle for health care
access and civil rights at home as more urgent and compelling. Ideally, all
progressive global health professionals, whether choosing a domestic or globally
focused path, will begin to address their own prejudices in new action-oriented ways.
There is a delicate but important balance between advocating for ongoing American
engagement in addressing global health inequities, while also addressing domestic
health care threats. One shouldn't be prioritized over the other or at the expense of
the other, as they represent two parts of the same global battle for health as a
human right that culminated in the Alma Ata Declaration, lost its way, and is
reemerging. Perhaps the real test will lie in America's response under the Trump
administration to the next Ebola, the next Zika, or the next HIV/AIDS epidemic.
AfricaFocus Bulletin is an independent electronic publication providing reposted
commentary and analysis on African issues, with a particular focus on U.S. and
international policies. AfricaFocus Bulletin is edited by William Minter.
AfricaFocus Bulletin can be reached at [email protected]. Please write to this
address to suggest material for inclusion. For more information about reposted
material, please contact directly the original source mentioned. For a full archive
and other resources, see http://www.africafocus.org
|

